Overview on Physiotherapy Management of Plantar Fasciitis.
Introduction
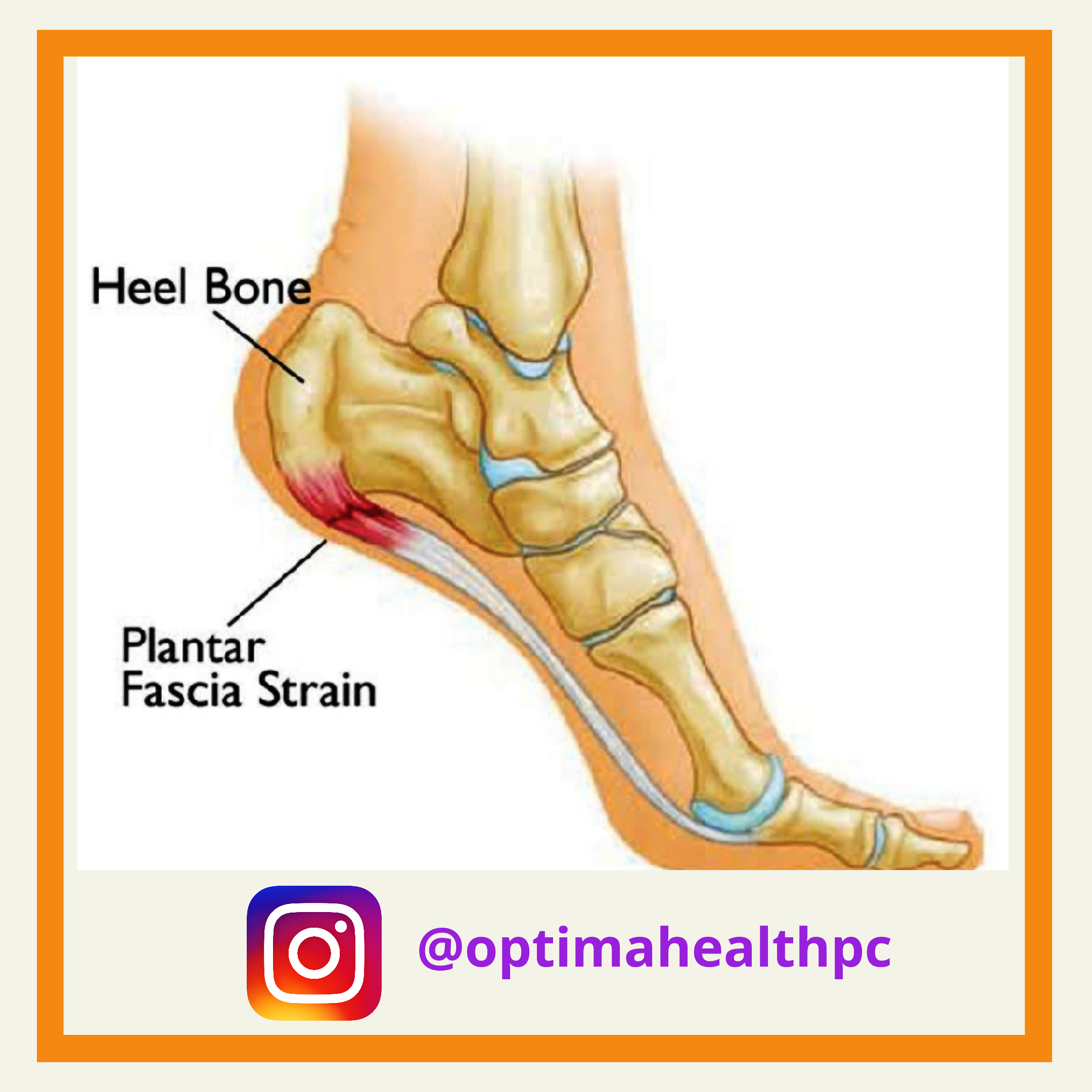
Plantar fasciitis (PF) is the common cause for heel pain affecting roughly 10% population. It is one of the common reasons for outpatient visits in a hospital. It was found that approximately 1 in 10 people will be diagnosed with PF during their life time with women aged 40-60 years most commonly affected. It affects both, people with sedentary lifestyle and athletic population due to chronic overload from lifestyle or exercises. The symptoms associated with plantar fasciitis are pain and tenderness on the inferior aspect of the calcaneus. Most of the cases respond to conservative treatment.
The plantar fascia is a dense, fibrous membrane spanning the length of the foot. It originates at the medial calcaneal tubercle, attaches to the phalanges, and provides stability and supports the arch of the foot. More recently, the term plantar fasciitis has been introduced to de-emphasize the idea that inflammation is the cause of pain.
Histopathologic studies have shown that patients with diagnosed plantar fasciitis have more disorganized fibrous tissue similar to degenerative tendinosis rather than inflammation. The most common symptom associated with plantar fasciitis is pain and tenderness on the inferior aspect of the heel, which is generally aggravated on weight bearing after an activity of non-weight bearing. There is intense pain in the heel after getting out of the bed in the morning but the pain subsides after walking few steps.
Extrinsic factors suggested include training errors, training on unyielding surfaces, and improper or excessively worn footwear. Intrinsic factors such as reduced plantar flexor muscle strength and flexibility, malalignment of foot with lower extremity and obesity. Also there is excessive pronation of foot seen in plantar fasciitis.
Decision making for treatment in PF can be challenging as there are lot of options available rather than a gold standard treatment. Generally recovery of PF takes about 6-8 months; early physiotherapy intervention has shown better results and has decreased the chances of surgery and injections. The treatment options include electrotherapy, stretching and strengthening exercises and use of orthosis or foot wear modifications.
Electrotherapy
The common belief about heat and cryotherapy is, heat is used in chronic conditions and cryotherapy is used in more acute conditions. In the acute stage of PF cryotherapy should be used as it will help in reducing inflammation of the tissue. Evidence have shown no inflammation in chronic PF, hence application of heat to the tissue may provide better results in treating PF.
Although there are evidences of therapeutic ultrasound, laser and iontophoresis being used as a treatment method for plantar fasciitis, the best results have been found with extracorporeal shock wave therapy (ESWT). ESWT uses pulses of high-pressure sound waves on damaged tissue to relieve pain associated with PF. It has been used as an alternative to surgery or those with chronic heel pain. The shockwaves cause micro disruption of the thickened plantar fascia, resulting in an inflammatory response, revascularization and recruitment of growth factors and therefore a soft tissue reparative response. It should be considered as a last treatment option, if other conservative treatment fails to work.
Manual Therapy
Manual therapy has also shown good results in treating PF. A multicentric study done by Cleland et al, have shown that manual therapy with exercises was superior to using electrotherapy in treating pain associated with PF. The intervention given to the patients differed according to patient’s signs and symptoms. As evidences show that there is associated ankle dorsiflexion restriction and pronated foot in patients suffering with PF, the authors tried to treat the positional faults associated with the poor biomechanics of the foot. The treatment given was soft tissue mobilization along with correction of positional fault.
Stretching and Strengthening Exercises
Stretching and Strengthening exercises play an important role in the treatment of PF. Generally there is tightness of gastrosoleus complex and plantar fascia along with weakness of intrinsic muscles of the foot is seen in patients with PF. Stretching and strengthening exercises will help maintain the normal posture of the foot thereby reducing the reoccurrence of PF. It has been found in studies that a 12 months regular exercise protocol followed twice/day have shown improvements in PF. Stretching exercises include, wall stretch, stair stretch, slant board stretch, towel stretch, rolling the foot arch on a ball, etc. Strengthening exercises should include more of intrinsic muscles of the foot. Exercises such as towel curls, toe taps, picking up marbles with toes etc should be included in the exercise program. Strengthening of the tibialis anterior has also shown to be beneficial in treating PF.
Taping, Orthosis and Shoes
Taping is a technique used for pain reduction in plantar fasciitis. There is a systematic review done on taping in PF, it has shown improvements in PF but the evidence is low. The techniques like the low-dye taping and calcaneal taping have shown to have better results as compared to placebo or no treatment, but this is temporary method as it does not address the pathomechanics in the foot. Studies have shown transient benefits of taping as even 24 mins of activity has shown to decrease the effect of taping.
Orthotics helps in more permanent effect as compared to taping. It helps to reduce load on plantar fascia while weight bearing, as it holds up the medial arch of the foot and reduces direct pressure on plantar fascia. An aperture on the orthotics can be useful in case of swelling of plantar fascia, as this will reduce the direct pressure on the heel. Orthotics would help to hold up the medial arch of the foot without placing any direct pressure of the ground on the plantar fascia. Also in a study the use of orthotics, including heel cups and plantar fascia support insoles, was found to be effective in decreasing pain from plantar fasciitis.
Literature shows that the prefabricated and custom made insoles are equally effective in decreasing the pain. There has been studies which have shown short term (3 months) effects of orthosis but long term effect have found to be ineffective. Shoes are also an important part while treating plantar fasciitis. Well fitted shoes are important; if they are ill fitted it may increase pain due to plantar fasciitis. It was found that using high-density ethylene vinyl acetate (such as is found in many running shoes), decreases the pain associated with long periods of walking or standing. Individuals with flat feet, there are options like motion control shoes or better longitudinal arch support, have helped to reduce pain due to PF. There has been a study where 14% patients showed improvement in pain by change of shoes. Thus studies have shown that 90%-95% cases of plantar fasciitis resolve within 12-18 months of conservative treatment. Conservative treatment is the choice of treatment in most of the cases. The combination of above treatment options can be best used to treat cases of plantar fasciitis and can be helpful in treating most of the cases.
